
Congenital orofacial anomalies require precise ICD-10 codes to report cleft lip and cleft palate to ensure accurate claims submission and proper reimbursement. Each type—whether isolated cleft lip, cleft palate, or combined presentations—has unique coding requirements that directly affect payer review, claim acceptance, and compliance verification.
Incomplete or unclear documentation, unspecified laterality, or incorrect combination code selection can trigger claim denials, delays, and additional payer queries. With increasing scrutiny from both commercial insurers and government programs, maintaining clean claims with correct ICD-10 codes is essential for efficient revenue cycle management.
To navigate this complexity, many practices utilize AI-driven medical coding services. These solutions combine automated rule checks with certified coder review to identify documentation gaps, validate code specificity, and align claims with payer coverage policies. This approach helps reduce rework, strengthen audit readiness, and protect revenue recovery for congenital anomaly billing.
Common Coding Challenges for Cleft Lip and Palate Claims
Claims for congenital facial anomalies require precise ICD-10 coding due to the complexity of anatomical variations and payer coverage rules. Accurate reporting depends on identifying whether the lip, palate, or both are involved, along with specifying laterality and the exact structural components affected. Even small gaps in documentation can alter code selection and trigger payer reviews, rework, or reimbursement delays.
The most common coding challenges include:
- Laterality specification: Claims must clearly indicate whether the cleft is unilateral, bilateral, or median. Missing laterality forces the use of unspecified codes, which increases denial risk and may delay claim adjudication.
- Combination code selection: When cleft lip and cleft palate occur together, coders must apply Q37 series combination codes rather than reporting separate Q35 and Q36 codes. Incorrect use of individual codes can result in claim rejections or payment reductions.
- Congenital sequencing accuracy: Cleft-related diagnoses must be sequenced according to ICD-10 congenital guidelines to ensure correct payer recognition of the primary defect and associated anomalies. Improper sequencing can trigger payer edits and post-payment audits.
- Incomplete clinical documentation: Missing details in operative reports, consult notes, or imaging summaries can prevent coders from selecting the most specific code and often result in requests for additional documentation or claim delays.
- Post-operative versus congenital diagnosis confusion: During follow-up or corrective encounters, payers may flag claims when congenital anomaly codes are reused without documentation reaffirming congenital status. This can lead to coverage denials or classification of services as non-covered cosmetic procedures.
Understanding these nuances helps ensure accurate coding and smoother claim adjudication while supporting compliance requirements.
Key ICD-10 Codes and When to Use Them
Accurate reporting of congenital facial anomalies depends on selecting the most specific ICD-10 codes. The type of cleft, its laterality, and whether the lip, palate, or both are involved all influence payer recognition and claim acceptance.
ICD-10-CM coding for cleft anomalies includes:
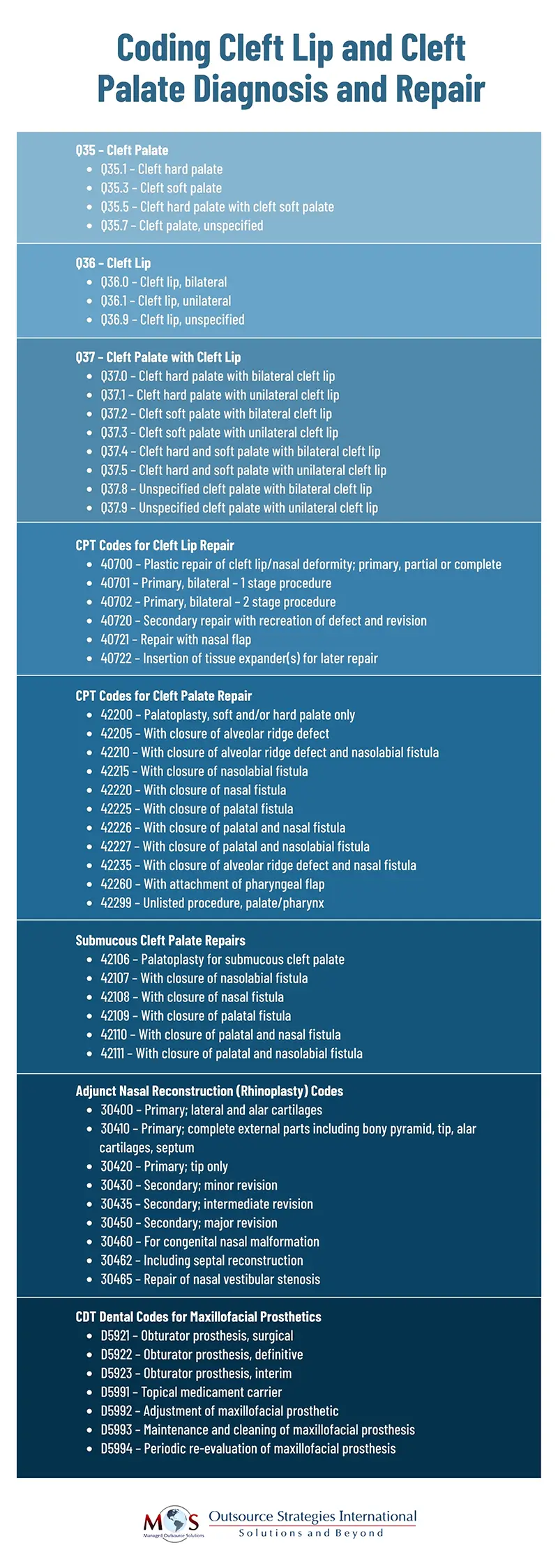
Cleft Palate (Q35 Series)
- Q35.0 — hard palate, bilateral
Use when both sides of the hard palate are affected. - Q35.1 — hard palate, unilateral
Use when only one side of the hard palate is involved. - Q35.3 — soft palate
Use when the defect involves the soft palate only. - Q35.5 — hard and soft palate
Use when both the hard and soft palate are affected. - Q35.7 — uvula
Use for isolated uvular clefts; this code is uncommon and should be supported by explicit documentation. - Q35.9 — palate, unspecified
Use only when documentation does not specify the anatomical extent of the palate defect.
Cleft Lip (Q36 Series)
- Q36.0 — Bilateral lip
Use when both sides of the lip are affected. - Q36.1 — Median lip
Use when the defect occurs in the midline. - Q36.9 — Unilateral lip, unspecified side
Use when documentation confirms unilateral involvement but does not specify right or left.
Cleft Palate with Cleft Lip (Q37 Series – Combination Codes)
When both cleft lip and cleft palate are present, Q37 combination codes must be reported instead of separate Q35 and Q36 codes. These codes capture the full scope of the anomaly and are required for accurate payer recognition.
- Q37.0 — Hard palate with bilateral lip
- Q37.1 — Hard palate with unilateral lip
- Q37.2 — Soft palate with bilateral lip
- Q37.3 — Soft palate with unilateral lip
- Q37.4 — Hard and soft palate with bilateral lip
- Q37.5 — Hard and soft palate with unilateral lip
- Q37.8 — Unspecified palate with bilateral lip
- Q37.9 — Unspecified palate with unilateral lip
Using the appropriate combination codes ensures claims reflect the complete congenital presentation, reduces the risk of payer edits, and supports accurate reimbursement for cleft-related services.
ICD-10 Documentation Guidelines for Pediatric Cleft Conditions
For cleft lip and palate claims, precise documentation is critical to support code selection and ensure payer approval. Coders rely on clinical records to confirm the type of anomaly, laterality, and whether multiple structures are involved. Missing or vague details often result in claim delays or requests for additional information.
Key documentation elements include:
- Type of defect: Clinical notes must clearly indicate whether the lip, palate, or both structures are affected. This distinction determines whether individual or combination codes are required.
- Laterality: Documentation should specify unilateral, bilateral, or median involvement. Missing laterality often forces the use of unspecified codes, which increases denial exposure.
- Palatal involvement: Records must differentiate between hard and soft palate involvement when applicable. This supports correct code selection and prevents payer misclassification.
- Congenital status confirmation: Providers should document that the condition is present at birth, even during later corrective encounters. This prevents payers from reclassifying services as cosmetic or non-covered.
- Procedure intent and clinical relevance: Notes should explain the medical purpose of related procedures or evaluations without detailing surgical techniques. This supports medical necessity and strengthens audit defensibility.
Clear, structured documentation improves coding accuracy, reduces rework, and supports faster claim adjudication while protecting compliance during payer review.
Best Practices for Coding Cleft Lip and Palate in Pediatric Patients
Accurate coding for congenital facial anomalies requires a structured approach that align documentation with ICD-10 specificity. Best practices help coders reduce errors, support payer compliance, and streamline claim submission.
Key practices include:
- Confirm laterality and combination rules: Coders should always verify whether the defect is unilateral, bilateral, or involves both the lip and palate before selecting a code. When multiple structures are affected, Q37 combination codes must be applied to reflect the complete presentation and prevent payer edits.
- Map documentation to payer policies: Clinical notes should be reviewed against payer-specific coverage rules and local coverage determinations. This ensures that assigned codes align with medical necessity requirements and reduces the risk of audits.
- Limit reliance on unspecified codes: Unspecified diagnosis codes should be used only when clinical documentation lacks required detail. Routine use of unspecified codes increases risk of rejections and may trigger additional documentation requests.
- Apply congenital sequencing standards: For encounters involving multiple anomalies, coders must follow ICD-10 sequencing guidelines to ensure that the primary defect is correctly identified. Improper sequencing can affect coverage recognition and reimbursement outcomes.
- Use peer reviews for complex cases: Encounters involving multiple structural variations or staged corrective procedures should undergo secondary review. Focused internal audits help identify inconsistencies and prevent denials.
Following these practices ensures claims are accurately coded, supported by documentation, and aligned with payer expectations, ultimately reducing denials and administrative burden for congenital condition billing. For accurate and timely medical billing and claims submission, healthcare practices can outsource their medical coding to a professional otolaryngology medical billing company that provides the services of experienced AAPC-certified coders.
Need help with cleft lip and palate medical coding?
Our certified coders specialize in pediatric ENT billing and congenital anomaly claims.

More from This Author


