Regarded as one of the most common and serious valve disorders, Aortic valve stenosis (also called aortic stenosis) occurs when the heart’s aortic valve narrows. The aortic valve – a key valve in the body’s blood circulation system – opens to...
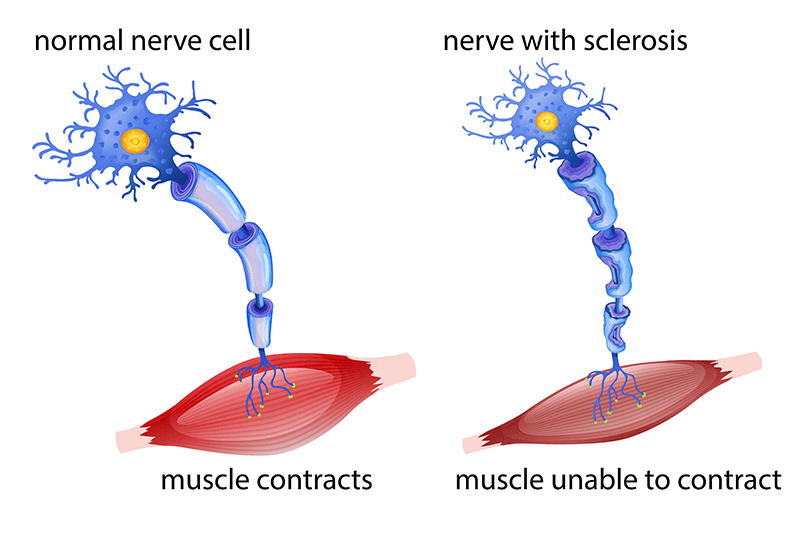
Primary lateral sclerosis (PLS) is a rare, neuromuscular disorder that affects the central nervous motor neurons (also called corticospinal neurons) and causes them to slowly break down. The condition may lead to painless but progressive weakness and stiffness of the...
Head injury is a serious condition that requires immediate medical attention. Generally, a person suffering from a head injury may not initially experience any feelings of being sick, but bleeding can occur within the skull. Internal bleeding can lead to serious...
Medical coding for cleft lip and cleft palate deformities can be a challenging process. For accurate and timely medical billing and claims submission, healthcare practices can outsource their medical coding tasks to an established medical billing company that provides...
Pressure ulcers/injuries are a common adverse event that medical coding companies help physicians report. The codes for pressure ulcers and non-pressure chronic ulcers are located in ICD-10 chapter 12, Diseases of the skin and subcutaneous tissue (L00-L99). Coding...

![Coding Cleft Lip and Cleft Palate Repair [Infographics]](https://www.outsourcestrategies.com/wp-content/uploads/2018/08/coding-cleft-lip-cleft-palate-repair.png)
