The financial health of a medical practice directly influences its capacity to invest in the latest medical technology, provide ongoing staff training, and deliver optimal care. Modern patients expect personalized treatment, a smooth billing experience, and...
As healthcare organizations grapple with financial challenges due to rising costs, declining reimbursement rates, and staffing shortages, proper revenue cycle management (RCM) has become more important than ever. RCM comprises various steps from patient intake to...
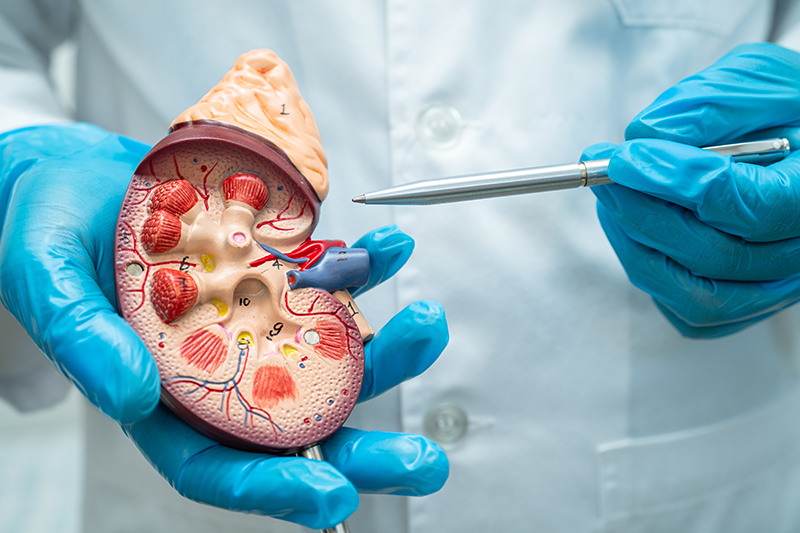
Glomerulonephritis (GN) is a chronic kidney disease (CKD) characterized by inflammation of the glomeruli – the tiny filters in the kidneys that filter waste and excess fluids. The excess fluid and waste that glomeruli remove from the bloodstream exit the body as...
Thyroid disorders include a wide range of conditions affecting the thyroid gland. Managing patients with thyroid disorders requires a comprehensive approach that includes accurate diagnosis, appropriate treatment, and long-term monitoring. Common thyroid disorders...
As physicians focus on providing individualized care for addiction, they also need to ensure precise documentation, proper coding, and accurate billing to reflect the services provided. Although most health insurance plans cover mental health and substance abuse...