
Stress is commonly seen as a normal response to life’s challenges. However, when it becomes persistent, it can contribute to physical, mental, and behavioral disorders, making its clinical impact more significant than often assumed.
In the U.S., nearly half of adults experience at least one traumatic event. Post-Traumatic Stress Disorder affects about 3.5% of adults each year and nearly 7% over a lifetime, often leading to functional impairment and coexisting with conditions like anxiety and depression. This highlights the importance of accurate documentation and ICD-10 coding to support care, ensure compliance, and optimize reimbursement. Specialized medical coding services that combine expert oversight with AI-assisted tools can help simplify claim submission for stress disorders.
Simplify Stress Coding
Leverage AI + certified coders to cut errors, speed reimbursements, and stay compliant.
This post outlines key ICD-10 psychiatric diagnosis coding guidelines, documentation best practices, and compliance tips for stress-related disorders.
Understanding Stress and Stress-Related Disorders in ICD-10
According to the DSM-5, stress-related disorders are classified under “Trauma- and Stressor-Related Disorders,” a category focusing on conditions where a clear stressful event causes significant psychological distress.
How Stress Impacts Physical and Mental Health
Stress becomes clinically significant when demands exceed an individual’s coping capacity, causing prolonged activation of the body’s stress response and affecting both physical and mental health. It can impact multiple systems, including cardiovascular, digestive, immune, musculoskeletal, and endocrine functions. Behaviorally, chronic stress is associated with anxiety, depression, sleep disorders, acute stress disorder, and PTSD, along with other functional impairments.
Key drivers include chronic stressors (work pressure, financial strain, relationship issues, chronic pain), trauma, and psychological factors such as perfectionism, pessimism, and low self-esteem.
Key Categories in the F43 Code Range
The ICD-10 code range F43 covers “reaction to severe stress and adjustment disorders.” These conditions arise from significant stress and include acute stress reaction, Post-Traumatic Stress Disorder (PTSD), and adjustment disorders, each distinguished by specific symptoms, duration, and severity.
Understanding these categories and features is essential for accurate diagnosis, documentation, and coding.
Common ICD-10 Codes for Stress Disorders
The ICD-10 code range F43 is used to classify reactions to severe stress and adjustment disorders, including conditions such as acute stress reaction and posttraumatic stress disorder.
Primary Range – F43.0-F43.2 – Includes codes for acute stress reactions and adjustment disorders, which are primary diagnoses for situational stress.
- F43 – Reaction to Severe Stress and Adjustment Disorders
- F43.0 – Acute Stress Reaction: A transient, immediate, short-term response to severe stress (when symptoms develop within 1 month of a traumatic event and resolve quickly).
- F43.1 – Post-Traumatic Stress Disorder (PTSD)
- F43.10: Unspecified
- F43.11: Acute
- F43.12: Chronic
- F43.2 – Adjustment Disorders: Used for short- or long-term responses to identifiable stressors causing impairment in functioning.
- F43.20: Unspecified
- F43.21: With depressed mood
- F43.22: With anxiety
- F43.23: With mixed anxiety and depressed mood
- F43.24: With disturbance of conduct
- F43.25: With mixed disturbance of emotions and conduct
- F43.29: With other symptoms
- F43.8 – Other Reactions to Severe Stress
- F43.81: Prolonged grief disorder
- F43.89: Other
- F43.9 – Reaction to severe stress, unspecified: unspecified stress reaction.
- Distinguish Between Stress, Anxiety, and Adjustment Disorders
- Stress: Normal response to external pressures, not always coded unless clinically significant.
- Anxiety Disorders: Persistent, excessive worry with physiological symptoms.
- Adjustment Disorders (Acute Stress Reaction): Emotional/behavioral symptoms tied to identifiable stressors, within 3 months of onset.
- Code by Severity
- Mild, moderate, or severe classification impacts code selection.
- Duration (acute vs. chronic) must be documented for accurate coding.
- Using Unspecified Codes
- Use only when documentation lacks detail.
- Clinical Validation Requirements for F43
- Symptoms such as dissociation – Evidence of dissociative episodes, panic attacks, or other stress-related manifestations.
- Transient symptoms – Clear documentation that symptoms are short-lived or fluctuate, consistent with acute stress responses.
- Stressor linkage – Direct connection between the identified stressor and the onset of symptoms.
- Functional impact – Notes on impairment in social, occupational, or daily functioning.
- Symptom duration – Specification of whether symptoms are acute, persistent, or evolving into adjustment disorder or PTSD.
- Ancillary and Differential Codes
- Z56.0 Captures occupational stressors such as job loss.
- F41.0 Panic disorder
- Triggered by an identifiable stressor; includes clinically significant emotional or behavioral symptoms
- Symptoms arise within a defined timeframe and impair functioning
- Symptoms typically resolve within six months after the stressor ends
- Includes subtypes such as: With anxiety; with depressed mood; with mixed anxiety and depressed mood
- Identified stressor: Clear link between the stressful event and symptom onset.
- Symptom description: Notes on dissociation, panic attacks, avoidance, arousal, or re-experiencing.
- Duration of symptoms: Specify whether symptoms are acute, transient, or persistent.
- Functional impact: Evidence of impairment in social, occupational, or daily functioning.
- Transient features: Documentation of short-lived or fluctuating symptoms when applicable.
- Differential diagnosis: Rule out anxiety, depression, or dissociative disorders if stressor linkage is unclear.
Documentation should specify the acute nature and short duration of symptoms.
ICD-10 Coding Guidelines for Stress-Related Disorders
Understanding mental health coding guidelines is essential for assigning the right diagnosis codes:
To support coding within the F43 range documentation should demonstrate:
When reporting stress-related disorders (F43 range), it’s important to consider ancillary and differential codes:
Ancillary Codes: Additional codes should be used in conjunction with the main diagnosis codes (F43.0 and F43.2) when applicable. For example:
Differential Codes: Differential codes may better capture the clinical presentation if criteria for F43 are not fully met. These codes help distinguish stress reactions from other psychiatric conditions with overlapping symptoms. For example:
Used when recurrent panic attacks occur without a clear external stressor.
Diagnosing and Coding Adjustment Disorder (F43.2)
Specifying type, severity, and duration of Adjustment Disorder (F43.2), also known as Situational Stress or Acute Stress Reaction, is important to avoid overuse of the condition. General criteria for adjustment disorders coding in ICD-10 include:
ICD-10 requires symptoms to appear within one month of a stressor, while the DSM-5 allows up to three months. As a result of these differences and the flexible criteria, adjustment disorders are under risk of inconsistent use, especially when symptoms overlap with other mental health conditions.
Stress vs. Adjustment Disorder ICD-10 Coding
Understanding the difference between stress and adjustment disorder ICD-10 coding is essential for accurate diagnosis and proper documentation.
In ICD-10, “stress” alone is not typically assigned a diagnosis code. General stress or life stressors that lead to a diagnosable condition can be coded as mental disorders using the following codes:
Z73.3 Stress, not elsewhere classified
R45.7 State of emotional shock and stress, unspecified
When no specific mental disorder is confirmed, but symptoms are present, use:
R45.89 Other symptoms and signs involving emotional state
For coders to choose the appropriate ICD-10 code for stress, clinicians should provide detailed documentation the patient’s condition.
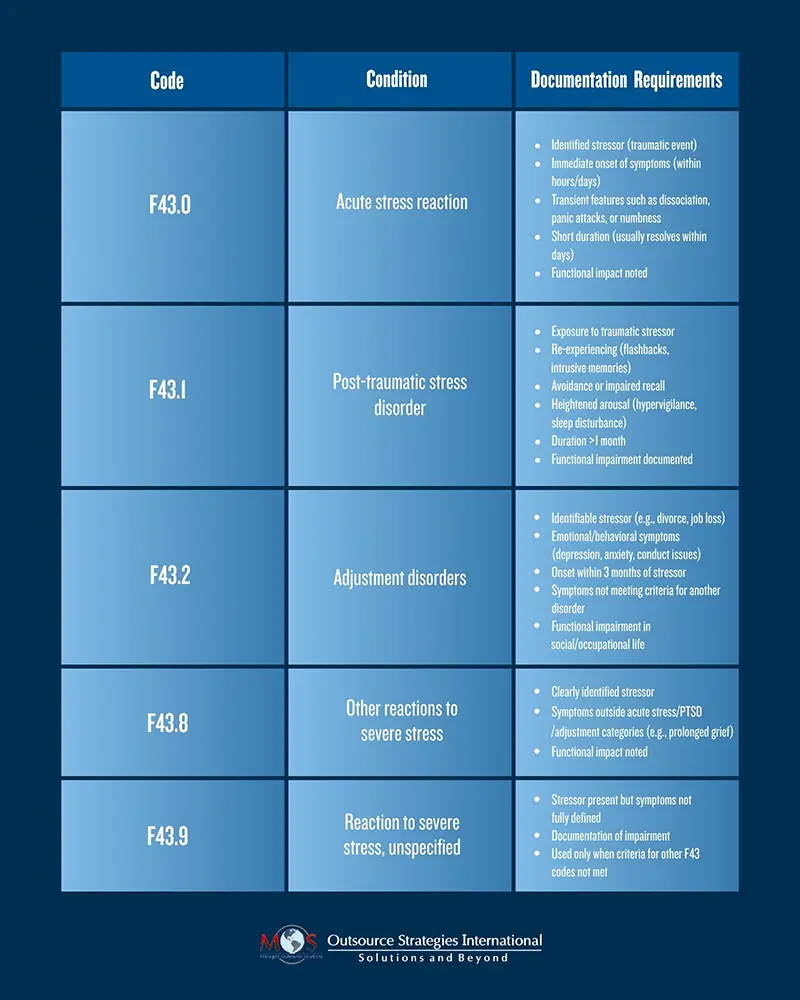
Documentation Requirements for Stress Disorder Coding ICD-10
The following table lists the essential elements of clinical documentation for stress disorders to ensure accurate ICD-10 F43 coding:
Simplify Stress Coding with AI + Human-in-the-Loop
An AI coding tool can streamline stress disorder coding by quickly identifying relevant F43 codes, flagging documentation requirements, and suggesting differential diagnoses.
When combined with medical coding outsourcing, organizations gain scalability and cost efficiency. Outsourced teams can handle volume while AI reduces repetitive tasks and human coders safeguard quality. This approach streamlines coding by reducing errors, improving efficiency, and maintaining the nuanced judgment required for mental health documentation.
Optimize Reimbursement
Boost your practice with expert medical coding services that deliver accuracy and efficiency.

More from This Author


